Prosperity as Health—Recentring Care to Guide Health System Reform
Tim Jackson
CUSP Working Paper Series | No 45

Abstract
Health systems are struggling not because they are failing, but because they are being asked to manage illness generated elsewhere. Across advanced economies, rising chronic disease, early onset multimorbidity and widening inequalities reflect the conditions in which health is produced, not simply the performance of healthcare.
This paper (commissioned for Enlighten’s NHS 2048 initiative in Scotland) argues that these pressures arise from a deeper misalignment between a wealth-centred model of prosperity and the requirements of human health. It explores how the social and material conditions of modern economies become biologically embodied over time, generating an unsustainable demand for healthcare.
In response, the paper proposes a reframing of prosperity as health and offers a simple policy test to distinguish reforms that reduce future harm from those that merely seek to absorb it. Recentring care as essential infrastructure becomes key to aligning policy with long-term health outcomes.
1 Introduction
Health systems across advanced economies are entering a period of sustained and intensifying pressure. High levels of chronic disease, the early onset of multimorbidity, persistent health inequalities and a growing strain on public health services have become defining features of the policy landscape.[1] These challenges are widely recognised and many countries have articulated ambitions around prevention, early intervention and person-centred care. Yet outcomes have not kept pace with intent.
Scotland provides a particularly clear and well-documented illustration of these dynamics. Higher than average prevalence of chronic disease and earlier onset of multimorbidity have been compounded by high levels of health inequality.[2] Such disparities have sometimes been dubbed the ‘Scottish effect’ or more locally the ‘Glasgow effect’—suggesting an unexplained gap between policy aspiration and health outcomes.[3]
This gap has generated a familiar response: a search for better evidence, improved implementation and more efficient service design.[4] While these efforts are necessary, they have not been sufficient. Despite repeated reform initiatives, prevention remains fragile, care struggles to gain institutional traction and demand continues to rise. Public health systems such as the National Health Service in Scotland absorb these pressures with remarkable commitment, but with diminishing room to manoeuvre.[5]
This paper starts from the premise that these difficulties cannot be understood—or resolved—through operational reform alone. They point instead to a deeper question about purpose: what the health system is ultimately being asked to do and how that task is shaped by wider policy choices. In particular, the paper argues that current debates underestimate the extent to which pressures on the NHS are generated outside healthcare and overestimate what medicine can reasonably be expected to offset.
Rather than offering another programme of recommendations, the paper seeks to reframe how choices about the reform of the health service is understood. It examines how prevailing assumptions about prosperity shape the conditions of life that produce health and illness over time, how those conditions translate into patterns of demand faced by public health systems and why care and prevention—despite repeated rhetorical endorsement—remain structurally marginal.
The analysis is not simply conceptual. It is aimed towards policy. Drawing on existing Scottish debates and examples, the paper explores what it would mean in practice to re-centre care as a core organising principle, rather than as a residual or discretionary activity. It argues that many of the necessary ingredients are already present, but that their impact is constrained by the absence of a consistent way to judge whether reforms alter the conditions that generate ill health or merely manage their consequences.
To address this need, the paper proposes a simple policy test to guide decision-making in relation to the reform of NHS Scotland. The test is not intended to rank policies or assess political intent. Its purpose is to make visible a distinction that is often implicit in reform debates: whether a given intervention contributes to reducing future harm and improving future health, or whether it primarily cushions the downstream costs of existing patterns of ill health.
The aim throughout is pragmatic. By clarifying choices rather than prescribing solutions, the paper seeks to support a more grounded debate about reform—one that recognises the limits of healthcare acting alone, the central role of care in sustaining health over time and the importance of aligning policy decisions with the kind of health system—and the kind of economy—Scotland wishes to lock in for the future. In other words, this paper argues, health reform must lie at the heart of the wellbeing economy.[6]
2 The Terrain of Health
Scotland’s health challenges are by now well-rehearsed. High levels of chronic disease, early onset of multimorbidity, stark health inequalities and growing pressure on NHS services have become familiar features of the policy landscape. What is less often acknowledged is that these challenges do not primarily reflect failures of clinical care. Nor should they be viewed as the aggregate result of poor individual choices. They are better understood as the predictable consequences of the social and material conditions in which people live over time: what might be described as the terrain of health.[7]
Health is often treated as a static state—something one either has or lacks.[8] But biologically, it is better visualised as a dynamic process. Living organisms survive and flourish by continually adapting to changing external conditions. Nutrition, stress, physical activity, housing quality, income security, social connection and time for rest and recovery all exert continuous influence on the body’s regulatory systems. When these systems are repeatedly pushed beyond their capacity to adapt, the result is not sudden collapse but gradual physiological wear and tear. Over time, this cumulative strain manifests as chronic disease.[9]
Physiology provides a useful language for understanding this process. The body maintains internal stability through mechanisms of regulation—what physiologists refer to as homeostasis.[10] When external pressures are occasional or short-lived, the body adapts and returns to balance. But when pressures are chronic—persistent stress, poor nutrition, insecurity, pollution—the body is forced into repeated adaptive responses.[11] The cumulative cost of these responses is known as allostatic load: the biological burden imposed by long-term exposure to adverse conditions.[12] As allostatic load increases, regulatory systems shift their set points. Metabolic control weakens. Inflammation becomes chronic. Resilience diminishes. Disease risk rises.
At the population level, these processes do not occur randomly. They follow social gradients. Where disadvantage is continuous rather than episodic, allostatic load accumulates earlier and more rapidly. In Scotland, this is visible in the well-documented pattern of early onset multimorbidity in more deprived communities. People experience multiple long-term conditions years earlier than their more affluent counterparts, often during what would otherwise be considered working age.[13] This pattern is not adequately explained by genetics, ageing or individual behaviour alone. It reflects the biological imprint of environments that are systematically misaligned with health over the life course.[14]
Seen in this light, chronic disease is not an aberration. It is not a failure of willpower, nor a failure of medicine. It is the embodied consequence of sustained exposure to hostile conditions. Disease becomes, in a sense, a signal: evidence that the terrain within which health is produced has been eroded.[15] This perspective does not deny the value of medical treatment. Nor does it imply biological determinism. It recognises instead that health is shaped long before individuals enter clinics or hospitals—and that the distribution of disease across society mirrors the distribution of disadvantage embedded in everyday life.[16]
This understanding has important implications for how we interpret demand on health services. Rising levels of chronic disease do not indicate that medicine has become less effective. On the contrary, modern healthcare has become extraordinarily successful at keeping people alive with long-term conditions. But when the terrain worsens or remains unchanged, success in treatment translates into rising prevalence and growing demand for ongoing care. The NHS finds itself managing the accumulated consequences of upstream failures over which it has little direct control.
To grasp the scale of the challenge facing public health services in advanced economies, it is therefore necessary to look beyond healthcare itself and examine the forces that shape this terrain in the first place. Those forces do not arise accidentally. They are shaped by the structures, institutions and norms embedded in society. In particular, they arise from the way in which prosperity is defined, pursued and measured across the economy. Understanding the impact of that overarching vision is essential.
3 Prosperity as Wealth
Every society operates with an implicit vision of prosperity. This vision is rarely debated explicitly, but it performs a powerful organising function. It shapes what is valued, what is measured, what attracts investment and what is treated as a cost. In contemporary political economies, prosperity is overwhelmingly framed in terms of wealth: rising GDP, productivity, profit and consumption are treated not merely as indicators of activity but as governing objectives in their own right.[17]
This framing does more than influence economic policy narrowly conceived. It shapes housing systems, labour markets, food production, urban design and time use. It privileges activities capable of generating scale, speed and financial return, while systematically undervaluing those that sustain balance, stability and wellbeing. In doing so, it exerts a quiet but decisive influence over population health long before healthcare enters the picture.[18]
When prosperity is equated with growth, the success of institutions is judged by how much they produce and how fast they expand. Work intensifies. Time becomes scarce. Productivity gains are pursued through speed, standardisation and control. These dynamics can sometimes deliver material abundance for some of the population. But they also generate insecurity, stress and inequality as structural by-products.[19] Stable livelihoods, secure housing, nourishing diets, clean environments and supportive social relationships—foundations of health over time—are often treated as constraints on expansion rather than as goals in their own right.
The result is a gradual erosion of the terrain of health. This terrain is not simply a backdrop to individual behaviour. It is actively shaped by policy choices, market incentives and institutional design. In Scotland, its degradation is visible in everyday conditions that are unevenly distributed across the population. Poor-quality housing exposes many households to cold, damp and mould, placing chronic strain on respiratory and cardiovascular systems. Insecure and low-paid work concentrates time pressure and stress, limiting opportunities for rest, recovery and care across the life course. Fuel poverty compounds material deprivation with physiological stress.[20]
Food environments provide a particularly clear illustration. In many Scottish communities—especially those facing higher deprivation—access to affordable, nourishing food is constrained, while energy-dense, ultra-processed products are readily available. These environments do not merely influence choice at the margins. They shape habitual diets in predictable ways, altering metabolic regulation and increasing the risk of obesity, diabetes, cardiovascular disease and poor mental health over time.[21] Such outcomes are not accidental. They are the foreseeable consequences of food systems organised around volume, shelf-life and price rather than nourishment.
It is worth noting that political support for ‘Big Food’—including ultra-processed food (UPF)—is significantly aided by the claims of the industry to offer an engine of economic growth.[22] But that same formula contributes to an epidemic of chronic disease. A recent study for the UK estimated the social costs of food-related chronic disease at £268 billion each year—almost twice the value of the food sector to the economy and four times the cost of ensuring that every person in the country could afford to eat well (Figure 1).[23]
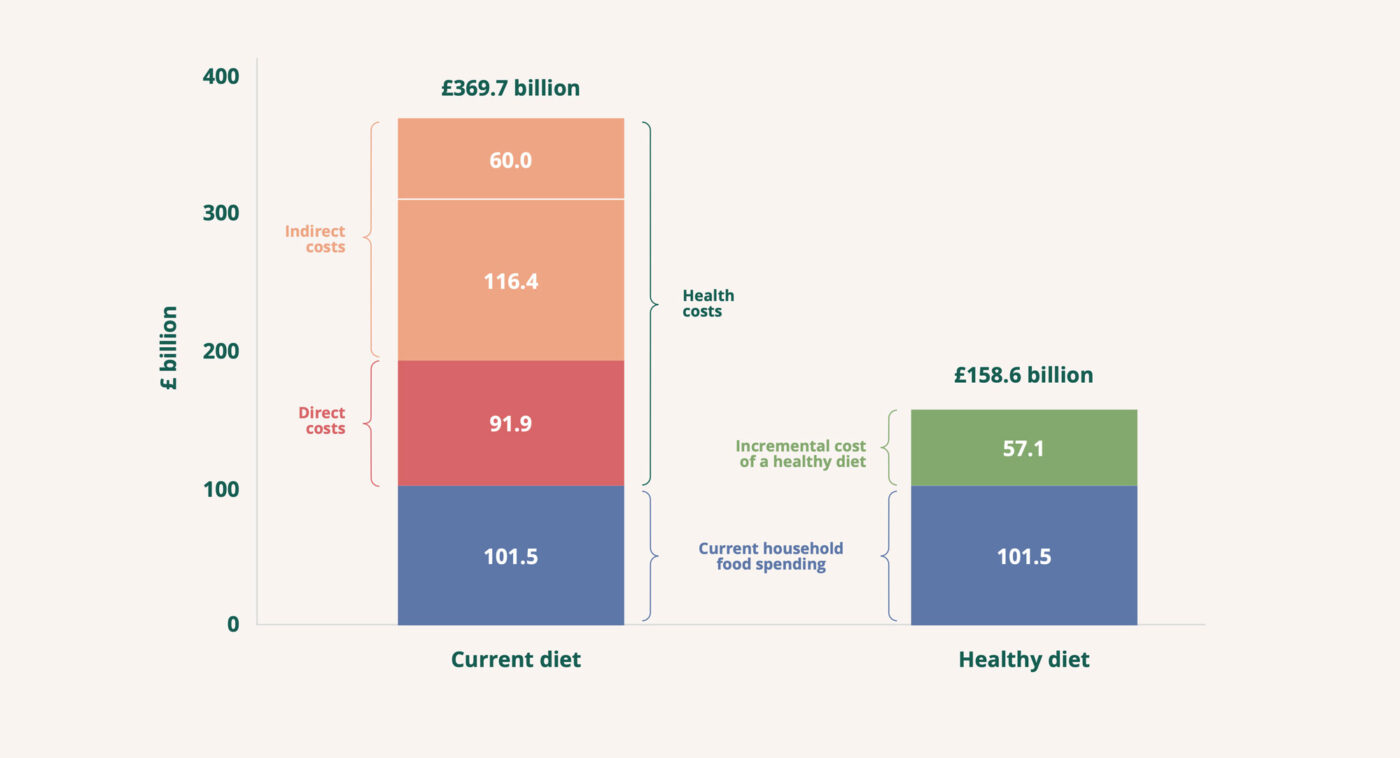 Figure 1: The economic costs of unhealthy vs health diets (source ref 23)
Figure 1: The economic costs of unhealthy vs health diets (source ref 23)
‘Big Pharma’ is quick to offer palliative responses to this damage and it too receives political support for its promise of growth.[24] But the unholy alliance of ‘Big Food’ and ‘Big Pharma’ does nothing to address the root causes of a broken food system. We end up with a ‘false economy’ whose rewards flow primarily into the pockets of shareholders and whose rising social costs threaten to overwhelm the public purse.
A comparable logic extends into the digital and algorithmic systems (including AI) which are increasingly embedded both at work and at home. Introduced primarily to increase efficiency and productivity, these systems often accelerate pace, intensify monitoring and compress time rather than freeing it. In doing so, they add new layers of cognitive load and chronic stress, reinforcing the same patterns of strain produced by other growth-oriented systems.
Crucially, the health impacts of these dynamics are socially patterned. Those with fewer resources have less capacity to buffer stress, gain access to healthier environments or avoid damaging conditions. Disadvantage becomes continuous rather than episodic. Over time, social gradients are translated into biological gradients. Inequalities become embodied. The resulting patterns of illness are neither random nor mysterious. They are cumulative, socially produced and deeply predictable.[25]
From this perspective, framing chronic disease primarily as a problem of individual behaviour or clinical management obscures its origins. Nor is it adequate to speak of “lifestyle” as though it were freely chosen. The terrain within which health is produced has been systematically reshaped by a wealth-centred vision of prosperity—and the consequences of that reshaping are now written into Scotland’s disease profile.
Once the terrain of health has been shaped in this way, healthcare systems inherit the consequences. If the NHS is struggling to cope with rising demand, this is not because it has failed to deliver care. It is because it has been positioned downstream of forces that continuously generate ill health. Medicine does not create these patterns of illness, but it is required to respond to them. It is at this point that the limits of a treatment-centred system become visible.
4 The Tragedy of Care
Unpacking the dynamics of prosperity as wealth is vital in understanding the demotion and denigration of care—not only within the health service but across society. The tragedy of care—and the systemic bias against prevention—do not arise because care and prevention are poorly understood, nor even because their importance is contested in principle. It arises because systems organised around accumulation and growth are structurally ill-suited to recognise, value or sustain the work of restoration on which health depends.
This misalignment operates through a combination of structural and normative bias. Structural bias arises through what economists call Baumol’s cost disease.[26] In care-intensive activities, productivity gains are inherently limited because the work itself depends on human time, attention and presence. A nurse cannot safely care for twice as many patients simply by working faster. A single GP cannot double the size of their list without compromising the doctor-patient relationship. A carer cannot provide meaningful support by halving the time spent with each person. The quality of care is inseparable from the time devoted to it.
In economies where prosperity is defined by productivity growth, this creates a systematic disadvantage for care-related activities. As productivity rises in sectors capable of automation, standardisation and scale, care appears increasingly costly by comparison. Its relative expense is interpreted as inefficiency, rather than as a reflection of the kind of work it involves. Funding systems, performance frameworks and investment decisions systematically favour activities that can demonstrate rising output per unit of labour, even when those activities do little to sustain health over time and sometimes militate against it.
This structural bias against care is reinforced by a powerful normative one. Care work has historically been feminised, informalised and moralised.[27] It has been associated with natural obligation, emotional labour and assumed availability rather than with skill, expertise or economic contribution. Much of it has taken place in households and communities, outside formal markets and beyond the reach of conventional economic accounting. It represents what the feminist author Nancy Folbre has called the invisible heart of the economy.[28]
Even when care is professionalised, these associations persist. They shape pay, status and authority within institutions. They influence which forms of work are seen as central to system performance. Medical intervention and technological innovation have tended to align more closely with masculinised norms of technical mastery, decisiveness and control—qualities that map easily onto institutional hierarchies and measures of value.[29]
Cultural patterns such as these help to clarify why prevention has remained so difficult to realise within wealth-centred systems. Prevention depends on the very capacities that growth-oriented systems struggle to sustain: continuity, long-term attention and the maintenance of conditions within which self-regulation remains possible. Prevention is inherently care-intensive and its benefits accumulate slowly over time rather than appearing as immediate outputs.
As a result, prevention consistently loses out within systems under pressure. Preventive initiatives are launched, piloted and often praised. But they remain vulnerable because they lack institutional protection. When acute demand rises—as it inevitably does in environments that continue to generate ill health—resources are drawn back towards visible intervention and crisis management. Prevention is deferred, fragmented or abandoned, not because it is ineffective, but because it depends on care in systems that do not reliably value or safeguard care.
In this sense, the failure of prevention is not an anomaly, an oversight or an accident. It is a predictable outcome of economies and institutions organised around growth and accumulation. Where there is no protected space for maintenance and restoration, systems become locked into managing breakdown rather than sustaining balance.
5 Prosperity as Health
The analysis so far points to a clear and uncomfortable conclusion. A wealth-centred vision of prosperity reshapes the conditions of life in ways that steadily erode health. That erosion becomes biologically embodied as chronic disease, which health systems are then required to manage downstream through medicine and pharmaceuticals. The result is a system that becomes ever more effective at treating illness while remaining structurally constrained in its ability to reduce the volume of illness it must treat.
At the core of this pattern lies not simply a failure of healthcare, but a failure of vision. Prosperity defined as wealth is organised around a particular dynamic: accumulation and growth. Success is measured by expansion—rising output, increasing throughput, continuous acceleration. Within this logic, there is no intrinsic point of sufficiency or balance. Systems are oriented towards movement rather than maintenance, towards pushing forward rather than holding steady. Once growth becomes the governing objective, it becomes difficult to recognise when limits have been reached, and harder still to slow down or reverse course once those limits are exceeded.
This dynamic matters profoundly for health, because health operates according to a fundamentally different logic. Health cannot be accumulated indefinitely. It cannot be maximised without constraint, stockpiled for future use, or expanded endlessly without consequence. Health is a condition of balance that must be actively sustained over time and restored when disrupted.[30] When prosperity is framed in terms of wealth, health appears as a cost—something that constrains productivity or requires expenditure. When prosperity is framed as health, that relationship is inverted: economic activity becomes a means to sustain balance rather than an end in itself.[31]
Prosperity as health begins from this different dynamic. Health, in this sense, is not the absence of disease, nor a state of optimisation or peak performance. It is the capacity of individuals and populations to maintain balance over time: to absorb shocks, adapt to changing circumstances and return towards equilibrium after disruption.[32]
This capacity for balance is not passive. Living systems possess an inherent tendency towards regulation and repair, but that tendency operates successfully only within certain limits. Physiological systems can adapt to stress, variation and challenge—but only up to a point. When pressures remain within tolerable bounds, recovery is possible. When those bounds are repeatedly exceeded—through chronic stress, deprivation, pollution, poor nutrition or insecurity—regulatory mechanisms become overwhelmed. The capacity to restore balance erodes, and the risk of breakdown increases.[33]
Prosperity as health therefore requires more than the avoidance of harm or the management of damage once it has occurred. It requires the active maintenance of conditions within which the natural propensity of living systems to restore balance can operate. Success is measured not by the volume of activity generated, but by whether social and economic arrangements sustain environments in which recovery remains possible and cumulative damage is avoided over time.
Seen in this way, prosperity as health reflects the realities of living systems at multiple scales. At the level of the body, health depends on homeostatic regulation: the continual adjustment of physiological processes to changing conditions. At the level of society, health depends on material security, time, social connection and supportive environments that allow people to live within tolerable bounds of stress and strain. At the planetary level, health depends on ecological balance and the integrity of the systems that sustain life itself. Without attention to these conditions, the capacity for self-regulation erodes, and health deteriorates even in the presence of advanced medical intervention.[34]
This shift in dynamic—from accumulation to balance—is central. Where growth-oriented systems struggle to recognise limits or to pause once they have been exceeded, a health-centred vision places limits, thresholds and resilience at the centre of decision-making. It asks not whether activity can be expanded, but whether it undermines or supports the conditions for continued adaptation and recovery.
The same shift has profound implications for the positioning of care and care work in the economy. If prosperity is understood as health and health depends on balance then care cannot remain marginal to economic purpose. Care is not simply a response to ill health after the fact. It is the work that sustains the conditions under which balance can be achieved and maintained in the first place.[35]
Care, in this sense, operates across several interconnected levels. At the most fundamental level, it involves maintaining the ecological conditions that sustain life on the planet: protecting the integrity of soils, water, climate and biodiversity within which human and non-human systems regulate and regenerate. At the level of the body, care supports the homeostatic processes through which physiological systems maintain equilibrium and recover from stress. At the level of social life, care involves the conscious, relational work through which people support one another to maintain the integrity of the material and social terrain within which health is produced.[36]
Across these levels, care is characterised by attentiveness, continuity and responsiveness to limits. It does not aim to eliminate fluctuation or disruption—both are inevitable—but to prevent fluctuation from becoming destabilising and disruption from becoming chronic. In doing so, care enables the inherent regulatory capacities of living systems to function effectively. Care functions as a vital restorative force: holding systems within the bounds where self-regulation remains viable.
Likewise, prevention becomes central to economic purpose. If prosperity is defined by the capacity of individuals and populations to maintain balance over time, then preventing the accumulation of allostatic load is not secondary to treatment; it is foundational. Investment in secure housing, nourishing food environments, time, income security, education and social connection is no longer justified primarily by downstream savings to healthcare budgets, but by its direct contribution to prosperity.[37]
This is the critical reordering implied by prosperity as health. Care and prevention cease to be framed as costs to be justified against growth. They become the primary means through which prosperity is pursued. Medicine retains its essential role in diagnosing and treating illness. But it no longer carries the impossible burden of compensating for environments organised against health.
Taken together, prosperity as health and economy as care describe a coherent alternative to wealth-centred models of success. They replace a logic of accumulation with a logic of balance. They replace a fixation on expansion with an orientation towards maintenance, repair and restoration. They do not reject economic activity, technology or medical innovation. But they reorder priorities, placing the work of sustaining the conditions for health at the centre of social and economic life.[38]
The challenge that follows from this reorientation is to find a way to embed it effectively and consistently within policy. That requires a test capable of distinguishing reforms that genuinely move institutions towards prosperity understood as health from those that merely cushion the costs of prosperity understood as wealth.
6 Policy Directions Consistent with Care
The preceding sections have argued that Scotland’s health challenges arise not primarily from failures of medicine or implementation, but from a deeper misalignment between how prosperity is understood and how health is produced. If prosperity is reframed as health, and if health depends on balance sustained over time, then care must move from the margins of policy to its centre. Many of the elements necessary for this shift are already present in Scottish policy debates. What is missing is a clearer organising logic: one that treats care as essential infrastructure, embeds prevention structurally and judges reform by whether it reshapes the conditions that generate ill health rather than merely managing its consequences.
Recentring care does not point to a single programme or blueprint. It implies a set of alignment choices: ways of realigning incentives, metrics, and institutional priorities so that care and prevention are no longer rhetorically endorsed but structurally embedded.
First, care must be treated as essential infrastructure, not as residual expenditure. Continuity, coordination, time, and relational support are foundational to managing chronic disease and multimorbidity, yet they remain vulnerable to erosion whenever systems come under acute pressure. Policy aligned with prosperity as health would protect care capacity explicitly, recognising continuity as a clinical asset rather than an inefficiency.
Second, performance and accountability frameworks must be rebalanced. What is measured shapes behaviour. Current regimes privilege throughput, access, and episodic activity. While these measures matter, they systematically obscure what sustains health over time. Embedding measures of continuity, coordination, and long-term outcomes—particularly for people with multiple long-term conditions—would help shift institutional attention from volume to durability.
Third, care roles across health and social care should be professionalised and elevated. Care work is skilled, outcome-critical labour, yet its status, pay, and progression rarely reflect this reality. Strengthening care roles, including coordination and boundary-spanning functions, is not ancillary to prevention; it is central to it.
Fourth, policy must recognise time as a therapeutic resource. Effective care for chronic disease requires time to listen, understand context, coordinate across services, and support change. Time spent on follow-up and relational work should be treated as legitimate clinical and care activity, not as lost productivity.
Fifth, upstream determinants that drive avoidable demand must be integrated into NHS sustainability planning.Food environments, for example, are powerful determinants of chronic disease, yet they are often treated as matters of individual behaviour rather than system design. Aligning food regulation, planning, and public procurement with health objectives—particularly for children and disadvantaged communities—addresses demand at source rather than downstream.
Sixth, policy should avoid reinforcing the false economy of chronic disease management. Pharmaceuticals deliver genuine clinical benefit, but prevailing incentives can normalise indefinite disease management where upstream prevention is feasible. Distinguishing clinical value from systemic lock-in is essential to preventing long-term dependency from crowding out care.
Seventh, prevention and care initiatives must move from pilots to permanence. Perpetual piloting fragments provision and undermines confidence. Where evidence supports impact, care and prevention models should be structurally embedded and protected from displacement during operational crises.
Finally, leadership should be framed around stewardship of population health. Success should be judged not only by operational recovery, but by progress in reducing future harm and moderating demand. Stewardship of health over time is not an optional leadership attribute; it is a core responsibility under prosperity understood as health.
These directions are not controversial in isolation. Many of them exist in some form both in the academic literature on healthcare and in policy prescriptions of one kind and another. What has been missing is a discipline for deciding whether policy choices genuinely move institutions in this direction, or whether they leave underlying dynamics intact. That is the purpose of the Policy Test proposed in the following section.
7 A Policy Test for Health Reform
The analysis set out in this paper leads to an uncomfortable but necessary conclusion. The difficulties experienced by advanced economies in addressing chronic disease, embedding prevention and sustaining their health services are not primarily failures of evidence, intent or professional commitment. They are symptoms of a deeper misalignment between how prosperity is understood and how health is produced.
This misalignment shapes what is valued, funded and protected when systems come under pressure. It helps explain why care remains marginal to institutional design even as its importance is repeatedly affirmed, and why prevention is persistently endorsed in principle but rarely embedded in practice. Both depend on time, continuity, stability and long-term investment in balance—precisely the qualities deprioritised in systems organised around productivity, throughput and growth.
For policymakers, the challenge is therefore not simply to identify effective interventions, but to decide what kind of system those interventions reinforce. This paper proposes a simple but powerful test to make that choice explicit:
- Does this intervention move institutions closer to prosperity understood as health—or does it merely cushion the costs of prosperity understood as wealth?
The policy test is intended as a decision discipline, not a scoring tool. It distinguishes between reforms that reduce the future production of ill health and those that primarily expand system capacity to absorb ill health already produced. It does not divide policies into “good” and “bad”. Measures that cushion the costs of ill health are often necessary, particularly in periods of acute operational pressure. But the test clarifies what such measures can and cannot achieve—and guards against mistaking stabilisation for reform.
At its core, the test asks whether policy acts upstream on the conditions of life, or whether it treats rising demand as fixed. It asks whether care is protected or squeezed when pressure increases; whether success is measured in sustained wellbeing or short-term activity; and whether future demand is likely to be lower, later, or less intense if the policy succeeds exactly as designed.
To clarify how this Policy Test operates in practice, Table 1 illustrates its application to a range of current or recent policy directions in Scotland.
| Policy direction | Primary policy intent | Performance against the policy test | Key risks and structural vulnerabilities |
| NHS operational recovery and improvement plans | Restore access, reduce waiting times, stabilise services | Predominantly cushions costs of ill health by expanding capacity and throughput; does not alter demand trajectory on its own | Becomes default mode of reform; crowds out care and prevention; rising demand treated as fixed |
| Primary care reform and Pharmacy First Scotland | Improve access, reduce pressure on GPs and acute care | Conditional: can reduce future harm if oriented toward continuity and proactive care; cushions costs if used mainly for diversion and throughput | Access without continuity accelerates activity; workload shifts without disease modification |
| Food environment regulation | Reduce exposure to unhealthy food environments | Strongly reduces future harm by acting upstream on a major driver of chronic disease | Benefits accrue slowly and are politically vulnerable; risk of dilution or delay |
| Care reform, integration, and National Care Service proposals | Address fragmentation, unmet need, and workforce instability | Conditional: aligns with prosperity as health only if it materially strengthens care capacity | Governance change without investment leaves care fragile; care squeezed during acute NHS pressure |
| Digital health, data reform, and AI initiatives | Improve efficiency, coordination, and decision support | Conditional and amplifying: can support care or intensify throughput depending on governance | Efficiency gains reinvested in activity; time compressed rather than freed; surveillance over care |
| Population health planning and strategic needs assessment | Shape service configuration and investment according to long-term epidemiology and inequality patterns | Conditional: reduces future harm if it redirects resources towards prevention; cushions costs if it primarily manages projected growth | Becomes descriptive rather than directive; lacks budgetary force; long-term allocation logic overridden by acute performance pressures |
| Performance and outcomes framework reform | Align measurement and incentives with continuity, coordination and long-term population health | Structurally decisive: advances prosperity as health if prevention and relational care are valued; cushions costs if throughput and access remain dominant metrics | Access and activity targets remain primary signals; prevention weakly measured; institutional behaviour defaults to volume and speed |
| Housing, fuel poverty, and energy efficiency policy | Improve living conditions and reduce household costs | Strong potential to reduce future harm by stabilising health terrain | Health impacts often treated as secondary; benefits sit outside health budgets |
| Work, time, and employment policy | Support economic participation and productivity | Conditional: can protect health if it stabilises time and security; undermines health if it intensifies work and stress | Productivity logic overrides health; stress and insecurity embedded as normal |
Table 1: Application of the policy test across a range of Scottish policy proposals
The policies shown in Column 1 of Table 1 are consistent with several strands of health and social care reform, including proposals articulated in the Service Renewal Framework (2025–2035).[39] They are not presented here as an exhaustive catalogue but as a representative set of strategic levers and directions through which the system is presently seeking to rebalance access, prevention, community capacity and efficiency.
The results of the test (Column 3 in Table 1) show whether the policy directions primarily cushion costs, promote prosperity as health or are conditional on their implementation. Column 4 in the Table identifies the key risks and vulnerabilities associated with each policy direction when seen from the perspective of prosperity as health. Several distinct patterns emerge.
Much of the reform agenda within NHS Scotland is necessarily focused on recovery: reducing long waits, stabilising workforce pressures and improving operational performance. These measures are often indispensable. But they tend to assume rising demand as given, responding through additional activity or ‘improved efficiency’ rather than by reshaping the terrain that produces ill health. When judged against the policy test, they largely cushion costs rather than alter causes.
By contrast, policies that intervene directly in the conditions of life—particularly those that reshape environments rather than relying on individual behaviour change—more clearly align with prosperity understood as health. Measures to improve food environments, for example, clearly work upstream of clinical demand. They reduce exposure to known drivers of chronic disease and in doing so reduce the need for medical intervention downstream. Their effects are slower and less visible than additional treatment capacity. But the impacts accumulate over time and have demonstrable potential to reduce future harm and improve population health.
Between these two poles sits a number of reforms whose impact depends heavily on how they are designed and governed. Investment in primary and community care, proactive outreach to people at high risk of chronic disease, digital and algorithmic systems (including AI) all have the potential to strengthen continuity, coordination, and long-term support. When such reforms are oriented towards sustained relationships and consistent follow-up, they can reshape demand and slow disease progression. But when they are oriented primarily towards access, speed and throughput, they risk being absorbed into the same intervention-heavy logic they were intended to relieve.
The same is true of reforms to care and integration. Structural change to governance or accountability can be important, but on its own it does not guarantee better care. Reforms pass the policy test only when they result in materially strengthened care capacity: improved conditions for the care workforce, greater continuity for people with complex needs, and stronger protection for care activity when systems come under pressure. Without this, reorganisation risks becoming an expensive rearrangement that leaves underlying dynamics untouched.
Proposals for new workforce models also fall into this conditional category. In fact, the role of work is a vital element in the care economy—both in and beyond the formal healthcare sectors. The conditions of work in care-related occupations are particularly vulnerable to attack—partly from escalating demand and partly as a result of the structural and normative pressures identified earlier in the paper. These pressures can easily be intensified by policy reforms focussed on narrow measures of productivity, which contribute to poorer working conditions and rising stress. On the other hand, measures that protect relational work, stabilise time and support economic participation could act to alleviate stress, improve the conditions of care and reduce future demand from ill health.
In summary, what this analysis reveals is not a failure of will or a lack of opportunities but a persistent tension. Scotland’s strategic frameworks consistently articulate a commitment to prevention, person-centred care, integration and reducing inequalities. Yet many of the mechanisms through which policy is delivered—funding flows, performance metrics, professional hierarchies and crisis-driven decision-making—continue to reflect a wealth-centred vision of prosperity, in which success is measured by activity and output rather than sustained health.
Making this tension explicit is the first step towards resolving it. The policy test does not demand that every intervention act upstream, nor does it deny the necessity of operational recovery. It does, however, require honesty about what different kinds of policy can achieve. Measures that cushion the costs of prosperity as wealth may be unavoidable in the short term. But they should not be mistaken for reform.
Reform, in the stronger sense, begins when economic and social institutions are progressively realigned around prosperity understood as health: when care is treated as infrastructure rather than residual expenditure; when environments that generate ill health are actively reshaped; and when success is measured by reduced future harm rather than better management of present demand. Scotland already possesses many of the policy ingredients for such a shift. The challenge now is to apply them consistently—and to judge new proposals not only by how they perform today, but by what kind of health system they lock in for tomorrow.
8 Conclusion: Governing for Health
This paper has argued that the pressures facing health systems in advanced economies cannot be understood—or resolved—through operational reform alone. Rising demand, chronic disease and widening inequalities are not simply challenges of delivery or efficiency. They are the downstream consequences of a dominant vision of prosperity organised around wealth, growth and accumulation. This vision systematically erodes the conditions required for health over time.
Seen through this lens, the NHS appears not as a failing institution but as a system increasingly required to absorb harm generated elsewhere. Medicine has become highly effective at managing illness once it appears. Yet it is structurally constrained in its ability to reduce the volume of illness it must treat. Care—the work of maintaining balance, enabling recovery and sustaining the conditions for health—remains marginal to how prosperity is conventionally measured, rewarded and governed.
The alternative set out in this paper is not simply another programme of reform. It is a call for a shift in organising principle. Prosperity understood as health reorients attention from accumulation to balance and from short-term output to long-term resilience. An economy oriented towards care recognises that health depends on the sustained maintenance of the ecological, biological and social terrain of health and that this work is economically foundational rather than residual.
The applied examples demonstrate that this distinction is not abstract. Policy choices already made—and those currently under consideration—align differently depending on whether they act upstream to reduce the production of ill health or downstream to manage its consequences. In the absence of an explicit decision discipline, systems organised around growth and throughput tend to default towards downstream absorption—even where upstream alternatives are available.
The policy test proposed in this paper offers a way to make that choice visible. It does not eliminate the need for judgement. Nor does it deny the necessity of stabilisation under pressure. It does, however, clarify what different kinds of policy can reasonably be expected to achieve and what kind of health system they are likely to entrench over time.
For policymakers, the implication is not that every reform must act upstream, but that the balance of policy effort matters. Without deliberate protection for care, prevention and the conditions of health, health services will continue to face rising demand regardless of how effectively they are managed. Governing for health therefore requires coherence across policy domains, patience with interventions whose benefits accrue over time and a willingness to judge success by reduced future harm rather than managed present pressure.
Scotland has long articulated ambitions for prevention, integration and reducing health inequalities. It also has a longstanding commitment to a wellbeing economy. The challenge now is alignment. The choice is between a rising tide of ill health which the NHS must continue to absorb at cost and the possibility of reform to improve and sustain the conditions through which people can remain well.
That choice is not technical. It is political, economic and moral. Making it explicit is the first step towards a healthcare system—and a society—that is organised not simply to treat illness, but to support health as the basis of shared prosperity.
Notes
[1] WHO 2023. Health for All: transforming economies to deliver what really matters. Geneva: World Health Organisation. https://www.who.int/publications/m/item/health-for-all–transforming-economies-to-deliver-what-matters
[2] SG 2024 The Scottish Health Survey 2024. https://www.gov.scot/publications/scottish-health-survey-2024-volume-1-main-report/documents/; Mercer et al (2024) Health inequalities, multimorbidity and primary care in Scotland. Future Healthcare Journal 10(3): 219-225. https://doi.org/10.7861/fhj.2023-0069.
[3] Spence, F 2024. The ‘Glasgow effect’: the controversial cultural life of a public health term. Medical Humanities 50: 60–69. https://mh.bmj.com/content/medhum/50/1/60.full.pdf.
[4] NHS Scotland 2025. NHS Scotland Operational Improvement Plan: https://www.gov.scot/publications/nhs-scotland-operational-improvement-plan/;
[5] McKirdy, M 2025. Independent Investigation into NHS Scotland. Scottish Labour: https://scottishlabour.org.uk/wp-content/uploads/2025/12/NHSScotland.pdf; see also Darzi, A 2024. Independent Investigation of the NHS in England. London: Department of Health and Social Care. https://www.gov.uk/government/publications/independent-investigation-of-the-nhs-in-england.
[6] Scottish Government 2025. Scotland’s Wellbeing Economy. Online at: https://www.gov.scot/publications/scotlands-wellbeing-economy/.
[7] The concept of the terrain of health has a long and sometimes contested pedigree in the history of medicine. It originated with the work of Antoine Béchamp in the late nineteenth Century as a way of framing susceptibility to infectious disease. It was picked up again in the mid-twentieth century by medical philosophers such as René Dubos (Dubos, R 1955. Second thoughts on the germ theory. Scientific American192(5): 31-5). The concept is perhaps most useful (and least contested) when it comes to understanding the burden of chronic, noncommunicable disease.
[8] For instance, the WHO defines health as ‘a state of complete physical, mental and social wellbeing and not simply the absence of disease or infirmity’ (https://www.who.int/about/governance/constitution.)
[9] Dubos, R 1959. The Mirage of Health—utopias, progress and biological change. New Brunswick, NJ: Rutgers University Press; Sterling, P 2020 What is health? Allostasis and the evolution of human design. Cambridge, MA: MIT Press; see also: Lustig, R 2021. Metabolical—the truth about processed food and how it poisons people and planet. New York: Harper Collins; Means, C 2024. Good Energy—the surprising connection between glucose, metabolism and limitless health. London: Harper Collins; Van Tulleken, C 2023. Ultra-processed People—Why Do We All Eat Stuff That Isn’t Food… and Why Can’t We Stop. London: Cornerstone Press.
[10] Cannon, W 1932. The Wisdom of the Body—how the body reacts to disturbances and danger and maintains the stability essential to life. New York: W W Norton; see also Dubos 1959 (ref 9).
[11] Sterling 2020 (ref 9); Sterling, P and J Eyer 1988. Allostasis: a new paradigm to explain arousal pathology. In S Fisher and J Reason (eds), Handbook of Life Stress, Cognition and Health. New York: John Wiley & Sons.
[12] Guidi, J et al 2021. Allostatic Load and Its Impact on Health—a systematic review. Psychotherapy and Psychosomatics 90(1): 11-27. https://pubmed.ncbi.nlm.nih.gov/32799204/.
[13] Finch, D, H Wilson and J Bibby. 2023. Leave no one behind—the state of health and health inequalities in Scotland. The Health Foundation. https://www.health.org.uk/health-inequalities-in-scotland-an-independent-review; see also Marmot, M et al 2022. Health Equity in England: the Marmot Review 10 years on. London: Institute of Health Equity.
[14] Lustig 2021 (ref 9); Means 2024 (ref 9).
[15] Dubos 1959 (ref 9).
[16] Finch et al (ref 13); Marmot 2022 (ref 13).
[17] Jackson, T 2017. Prosperity without Growth—foundations for the economy of tomorrow. London: Routledge. Jackson, T 2021. Post Growth—life after capitalism. Cambridge: Polity; Kallis, G et al 2025. Post-growth: the science of wellbeing within planetary boundaries. The Lancet Planetary Health 9(1). https://doi.org/10.1016/S2542-5196(24)00310-3.
[18] Jackson, T 2025. The Care Economy. Cambridge: Polity.
[19] WHO 2025. Social Determinants of Health. Geneva: World Health Organisation. https://www.who.int/news-room/fact-sheets/detail/social-determinants-of-health.
[20] Finch et al 2023 (ref 13).
[21] Lane, M et al. 2024. Ultra-processed food exposure and adverse health outcomes: umbrella review of epidemiological meta-analyses BMJ 384: e077310; doi:10.1136/bmj-2023-077310; Monteiro, C et al 2025. Ultra-processed foods and human health: the main thesis and the evidence. The Lancet 406 (10520): 2667-2684. https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(25)01565-X/; see also Lustig 2021 (ref 9); Means 2024 (ref 9).
[22] FDF 2025. Ingredients for Growth—driving growth in food and drink manufacturing. Food and Drink Federation. Available at: https://www.fdf.org.uk/fdf/resources/publications/reports/ingredients-for-growth-report/.
[23] Jackson, T 2024. The False Economy of Big Food. Food, Farming and Countryside Commission. Available at: https://ffcc.co.uk/publications/the-false-economy-of-big-food.
[24] WifOR 2024. The Economic Impact of the Global Pharmaceutical Industry. Available at: https://www.wifor.com/en/download/economic-impact-of-the-global-pharmaceutical-industry/.
[25] Finch et al 2023 (ref 13); Marmot et al 2022 (ref 13).
[26] Baumol, W 2012. The Cost Disease: why computers get cheaper and healthcare doesn’t. New Haven, CT: Yale University Press; Jackson 2025 (ref 18, Chapter 11).
[27] This case has been made by numerous authors over recent year, including Bunting, M 2020. Labours of Love: the crisis of care. London: Granta; Dowling, E 2021. The Care Crisis: what caused it and how to end it. London: Verso; Ehrenreich, B and D English 2010. Witches, Midwives and Nurses: a history of women healers. New York: The Feminist Press. Eisler, R 2007 The Real Wealth of Nations: creating a caring economics. San Francisco: Berret Koehler; Folbre, N 2001. The Invisible Heart: economics and family values. New York: The New Press; Gilligan, C 1982. In a Different Voice: psychological theory and women’s development. Cambridge, MA: Harvard University Press; Lynch, K 2022. Care and Capitalism. Cambridge: Polity; see also Jackson 2025 (ref 18, Chapter 12).
[28] Folbre 2001 (ref 27).
[29] Ehrenreich and English 2010 (ref 27); see also Jackson 2025 (ref 18, Chapter 12).
[30] Dubos 1959 (ref 9); see also: Mol A 2008. The Logic of Care: health and the problem of patient choice. London: Routledge.
[31] Jackson 2025 (ref 18); see also Jackson, T 2026. Prosperity as health—why we need an economy of care for a liveable future. BMJ2026; 392: r2573. https://doi:10.1136/bmj.r2573; Jackson, T and J Sheather. 2021. Why health should replace wealth as the heart of prosperity. BMJ Opinion 30th July 2021: https://blogs.bmj.com/bmj/2021/07/30/why-health-should-replace-wealth-as-the-heart-of-prosperity/.
[32] Cannon 1932 (ref 9); Dubos 1959 (ref 9); Sterling 2020 (ref 9).
[33] Sterling 2020 (ref 9); Sterling and Eyer 1988 (ref 11); Guidi 2023 (ref 12).
[34] Jackson 2025 (ref 18).
[35] Fisher, B and J Tronto 1990. Towards a feminist theory of caring. In E Abel and M Nelson Circles of Care: work and identity in women’s lives. New York: University of New York Press; Jackson 2025 (ref 18, Chapters 4 and 14).
[36] Jackson 2025 (ref 18, Chapter 4).
[37] Eisler 2007; see also: Jackson 2025 (ref 18, Chapter 15); WHO 2023 (ref 1).
[38] Mol 2008 (ref 30).
[39] Scottish Government 2025. Health and Social Care Service Renewal Framework 2025-2035. Edinburgh: Scottish Government. https://www.gov.scot/publications/health-social-care-service-renewal-framework/documents/.
Download
Jackson T 2026. Prosperity as Health— Recentring Care to Guide Health System Reform. CUSP Working Paper Series, No 45. Guildford: Centre for the Understanding of Sustainable Prosperity.
Acknowledgements
This working paper was commissioned as an input to Enlighten’s NHS 2048 initiative which aims to foster a mature cross-party debate on reforming Scotland’s health and social care system. The author is grateful for comments and suggestions on various drafts from Linda Gessner, Bryan Jones, Jen Morgan, Alison Payne, Jonathon Porritt, John Sturrock and the participants at a workshop held at the University of Surrey in January 2026.